




IN FOCUS: The rapid rise of the Delta variant and how it is shaping Singapore’s COVID-19 fight

A man wearing a protective face mask taking a photo at Jewel Changi Airport on Dec 8, 2020. (Photo: Calvin Oh)




SINGAPORE: On May 31, Prime Minister Lee Hsien Loong signalled that a new, dangerous front had opened up in Singapore's battle against COVID-19.
It was not about the tightening or easing of restrictions, but a shift in strategy to contain a changing enemy.
“Unfortunately, we are also fighting new, more infectious variants of the COVID-19 virus,” he said. “What does a more infectious virus mean for our fight against COVID-19? It implies that we must continually adjust our strategies and raise our game to keep COVID-19 under control.”
Singapore, Mr Lee said, needed to do more of three things, and faster: Testing, contact tracing and vaccination against COVID-19.
READ: Singapore 'on track' to bring COVID-19 outbreak under control; curbs may be eased after Jun 13: PM Lee
On Friday (Jun 18), Health Minister Ong Ye Kung said Singapore has raised its contact tracing, testing and quarantine capabilities as well as vaccinated a "good part" of its population.
“So I believe we are now able to put ‘circuit breaker’ behind us and keep most businesses open while navigating a wave of transmissions, as we have just done over the past few weeks,” he said.
But even as he signalled progress was being made, Mr Ong also sounded a cautionary note: “However, with the Delta variant, we still need to be very careful of high-risk settings, meaning enclosed, mask off, and lots of interaction, namely in F&B (places) and gyms.”
It is easy to see why the variants have created a new dynamic for the authorities to deal with.
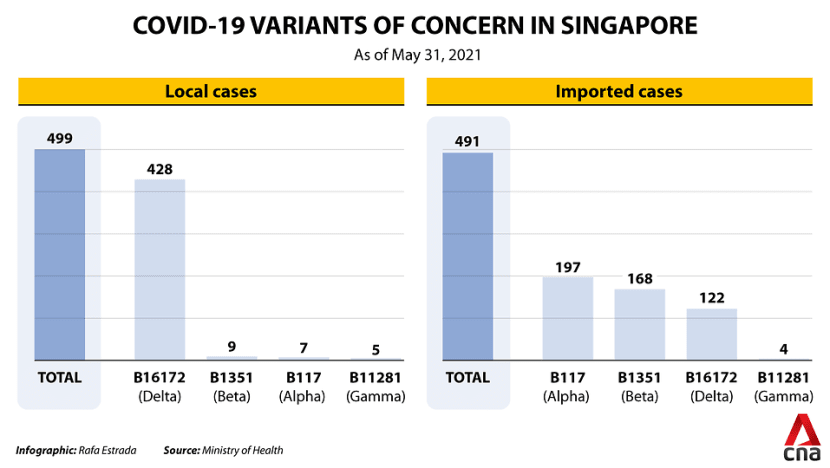
The Ministry of Health (MOH) told CNA on Friday that as of the end of May, it has detected 428 local COVID-19 cases with the more infectious B16172 variant – recently dubbed the Delta variant – of the coronavirus first detected in India.
The Delta variant has also been identified in 122 imported cases, MOH said.
The B1617 variant has been called a triple mutant variant since it is split into three lineages, including B16171 (Kappa) and B16172.
While MOH did not say when the first Delta variant case was confirmed in Singapore and which case this was, figures from the global epidemic tracker GISAID show that the first Delta case was detected here on Apr 1.
The GISAID data did not indicate if this first case was local or imported.
From Apr 1 to May 31, MOH announced in its daily updates a total of 574 new community infections.
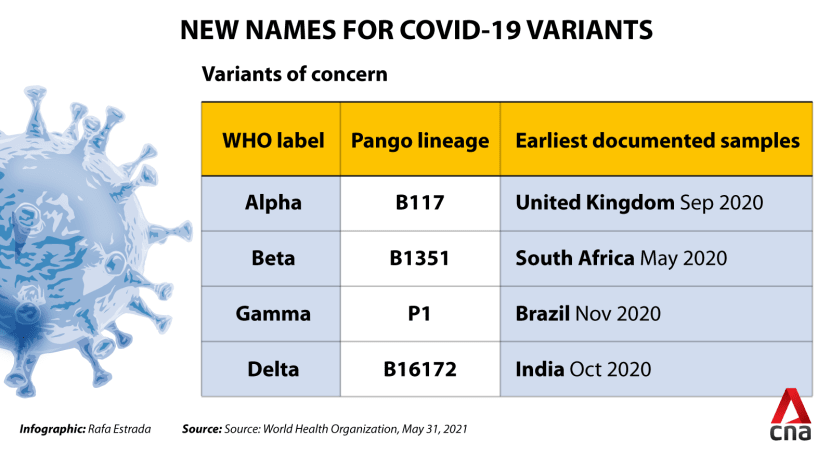
MOH figures also showed that as of May 31, nine local cases have the B1351 (Beta) variant first detected in South Africa, seven local cases have the B117 (Alpha) variant first detected in Britain, and five local cases have the B11281/P1 (Gamma) variant first detected in Brazil.
The World Health Organization (WHO) has identified these strains as “variants of concern” as they are more transmissible, virulent, or resistant to public health measures or treatments.
READ: Is it all Greek to you? COVID-19 variants get new names
MOH also said early in May that three local cases have the Kappa variant.
The Kappa variant is a “variant of interest” under WHO’s classification, meaning it has caused community transmission and clusters, or has been detected in multiple countries.
MOH said the National Public Health Laboratory conducts viral genomic sequencing on all COVID-19 cases in Singapore to detect variants.
“Sequencing and analysis takes about seven days on average but it may take longer, particularly if there is a lower viral load in the swab specimens,” a spokesperson said. “Due to the time taken to carry out this process, variant cases will be reported as confirmed cases, but not necessarily as variant cases, in our daily press releases.”
The spokesperson said sequencing is an ongoing process carried out concurrently with “prompt public health action”.
“The National Centre for Infectious Diseases (NCID) reports regularly to GISAID as and when the analysis is completed,” the spokesperson added.
CHANGI AIRPORT CLUSTER
The B1617 variant’s relentless spread was highlighted in the Changi Airport cluster, which ballooned to more than 100 cases in less than a month to become Singapore’s largest active COVID-19 cluster. The cluster was closed on Friday after going through two incubation periods without any new cases.
The cluster’s index case, Case 62873, is an 88-year-old cleaner who worked at Changi Airport Terminal 3. He tested positive on May 5 despite being fully vaccinated.
While it remains unclear how exactly the variant reached Singapore, spread so quickly and infected other members of the public, there were some early clues.
TIMELINE: How Changi Airport became Singapore's largest active cluster
Mr Ong Ye Kung said on May 14 that several cases linked to the airport cluster had tested preliminarily positive for the B1617 variant.
The infected airport workers mainly received travellers from high-risk countries in the immigration and baggage claim areas, he said. These workers would then go on to have their meals at the Terminal 3 Basement 2 commercial area and food court, where they likely passed the virus to the community, he added.
Initial transmission could have occurred through an airport worker who had helped a family from South Asia, the Civil Aviation Authority of Singapore and Changi Airport Group (CAG) said on May 21. The family later tested positive for the virus.

On May 24, CAG chief executive officer Lee Seow Hiang confirmed that the B1617 variant was part of what caused the cluster.
While the CEO said the airport had implemented “many layers of stringent safety protocols”, he acknowledged that “something changed” with the B1617 variant.
“It penetrated our defences and caused a community outbreak,” he conceded.
The Changi Airport cluster had 108 cases as of Friday, with the most recent cases reported on May 23.
OTHER NOTABLE CLUSTERS
Another large cluster linked to the B1617 variant was the one that spread in Tan Tock Seng Hospital (TTSH). This remains Singapore’s only COVID-19 cluster in a hospital. The cluster is now closed.
A fully vaccinated 46-year-old female nurse at TTSH, or case 62541, became the first case linked to the cluster after she tested positive on Apr 27.
By May 4, just a week after the first case was discovered, the cluster had swelled to 40 cases, MOH figures showed.
On the same day, MOH’s director of medical services Kenneth Mak confirmed that the nurse, along with four others in the cluster, were infected with the Delta variant. Authorities are still investigating the source of the cluster.
READ: A timeline of the Tan Tock Seng Hospital COVID-19 cluster
Until now, variant cases continue to emerge alongside new clusters.
MOH confirmed on Wednesday that one case in the new Bukit Merah View market cluster had tested preliminarily positive for the Delta variant. The cluster was first identified three days earlier on Jun 13 with four cases linked to the food centre there. The cluster had 65 cases as of Friday.

Assistant Professor Hannah Clapham, who researches infectious diseases at the National University of Singapore’s (NUS) Saw Swee Hock School of Public Health, said it was important to study the clusters to learn about the Delta variant’s transmission rate, where and how it was spreading, and the effectiveness of the measures against it.
“It would seem that the higher transmissibility of the B16172 variant did mean that it was able to evade the measures that were in place in Singapore,” she said.
“It could also be that as this variant was spreading globally, we saw more introductions of B16172 into Singapore and therefore this is the variant that spread.”
READ: Delta variant fuelled 50% rise in England's COVID-19 prevalence: Study
Other countries are also dealing with the new challenges presented by the more infectious variant.
According to GISAID, the UK had reported 46,890 Delta cases as of Friday, the highest number of confirmed cases in the world ahead of India (6,684 cases) and the US (2,853 cases).
The US Centers for Disease Control and Prevention on Tuesday recognised the Delta variant as a “variant of concern”, with top infectious diseases expert Dr Anthony Fauci encouraging everyone to get vaccinated, CNN reported. Dr Fauci pointed out that the Delta variant was in circulation in the United States at a rate similar to the tipping point seen in the UK, where the variant has become dominant.
The UK had announced on Monday that it would delay the easing of COVID-19 restrictions by another four weeks, until Jul 19, following a rise in cases and the growing spread of the Delta variant.
HOW MUCH MORE INFECTIOUS?
Beyond the fast rate of infection, it is worth understanding how variants form and how a particular strain gains dominance over the rest.
There are thousands of different coronavirus variants circulating worldwide. Viruses mutate all the time when replicating and most changes make no difference. Some even harm the virus.
But others can make the virus more infectious and the disease more threatening – and these strains tend to dominate.
“The few mutations that give a virus an advantage, such as being able to bind to the host cell better, tend to (allow the variant to) survive and eventually replace the other strains of the virus,” Dr Paul Tambyah, president of the Asia Pacific Society of Clinical Microbiology and Infection, told CNA.
So, while experts CNA spoke to agreed that the Delta variant is more infectious, how much more infectious exactly is it?
“PCR tests indicate that the amount of virus in the (Delta) samples is often higher than what we see before,” said Professor Leo Yee Sin, executive director at the NCID.
“This could be 100- to 1000-fold higher than expected, reflecting the millions of virus particles present in each specimen. This high viral load in the respiratory tract may imply higher transmission ability resulting in a large number of cases and at faster speed.”
Citing research coming out of the UK, Dr Tambyah said the Delta strain was associated with secondary infections in 13.5 per cent of cases with local transmission. This is in contrast to 11 per cent for the Gamma variant and 8.1 per cent for the Alpha variant.
AIRBORNE TRANSMISSION OF VARIANTS
Another worry is the potential airborne transmission of variants.
While it has been established that COVID-19 infection primarily occurs through exposure to respiratory fluids carrying the virus, the science increasingly shows that the virus could also be spread by tiny particles suspended in the air.
COVID-19 multi-ministry task force co-chair Lawrence Wong alluded to this on May 18 when recommending the wearing of masks with better filtration.
“It's not just wearing a cloth mask, but wear one with high filtration capability – a surgical mask or one of those with the filter inserts,” he said. “That is important because of the latest evidence about the nature of the various strains, how transmissible they are and the fact that the spread can happen through aerosolised particles.”
READ: Masks with better filtration capability recommended as new COVID-19 variants spread
Professor Laurent Rénia, who studies infectious diseases at Nanyang Technological University’s (NTU) Lee Kong Chian School of Medicine, said the issue of airborne transmission is still a matter of debate in the scientific community.
“But evidence is accumulating that short range aerosol transmission may occur,” he said.
NCID’s Prof Leo said the larger amount of virus excreted by Delta variant cases could be spread through various modes of transmission, including direct contact, surfaces and airborne droplets.
“When a person sneezes or coughs, he or she produces a range of particles of different size and weight,” she explained. “The very small and light particles can be dispersed a longer distance away and some might linger in the air for a longer period of time.”

Professor Dale Fisher, senior consultant at the National University Hospital’s (NUH) division of infectious disease, believes the variants’ more infectious nature makes it seem like transmission modes have changed.
“What might look like a change in the mode of transmission is actually just because the virus is less forgiving,” he said. “Now, if an aerosol could have transmitted it before uncommonly, well maybe now it might be a little bit more common.”
VACCINES EFFECTIVE AGAINST VARIANTS?
With the variants being more infectious and potentially spreading through the air, some have questioned how effective current vaccinations are against these strains.
Some studies have shown that vaccines are slightly less effective against the Delta variant, but the experts were quick to stress that the jabs still offered good protection and helped reduce severe disease.
For instance, Dr Leong Hoe Nam, infectious diseases specialist at the Rophi Clinic, pointed to a UK study that showed the Pfizer-BioNTech shot was 88 per cent effective against the Delta variant two weeks after the second dose. The Pfizer-BioNTech jab has a usual efficacy of about 95 per cent, meaning the chance of getting COVID-19 is 95 per cent lower after full vaccination.

In the Delta variant clusters, Prof Leo has seen vaccinated cases with family members who have tested positive. This means it could still be possible for vaccinated people to spread the virus.
“Genetic sequencing monitoring by the National Public Health Laboratory is still ongoing and we cannot rule out that a vaccinated patient is capable of transmitting the infection,” she said.
Still, Dr Tambyah said a vaccine effectiveness of at least 80 per cent was “more than enough to eliminate the virus eventually when enough people are vaccinated”.
“Vaccine breakthroughs occur with any virus, including the highly successful measles and chickenpox vaccines, but when enough people are vaccinated, the breakthroughs are rare and of limited public health significance,” he said.
Dr Tambyah said vaccines have shown “time and again” to be the only way to end an epidemic, including in smallpox and to a lesser extent polio and measles. “Careful vaccination strategies are needed to ensure that the community transmission of the virus in Singapore is significantly reduced,” he said.
Forty-nine per cent of the population have taken their first doses of vaccination, and “slightly over” 35 per cent are fully vaccinated with both doses, Mr Ong said on Friday. As of Jun 15, more than 4.7 million doses of the COVID-19 vaccination have been administered in Singapore, he added. More than 2.7 million people have received at least one dose of the COVID-19 vaccine.
READ: Singapore accelerates national COVID-19 vaccination programme, students the next group to be inoculated
READ: 'Overwhelming' response for Sinovac COVID-19 vaccine at some approved clinics
Still, the experts said Singapore’s vaccination strategy could evolve as more people got their jabs.
If evidence shows that the variants could “escape” the immune response induced by the vaccine or after natural infection, NTU’s Prof Rénia said a booster injection of a new vaccine with proteins from the variants could be necessary.
Dr Tambyah also pointed to the possibility of the authorities introducing “ring vaccination”, when contacts of a single case or small cluster are quickly vaccinated.
While this approach has yet to be tried in the COVID-19 pandemic, it proved effective in mumps outbreaks on US college campuses, he said. “It may not work for secondary cases but it will reduce further spread,” he added.
TESTING AND CONTACT TRACING
Vaccination is just one brick in the wall keeping COVID-19 variants at bay. Testing and tracing strategies are set to evolve as the vaccination rollout progresses, the experts said.
Routine and large-scale testing for COVID-19 could become part of Singapore’s new normal. Singapore is shifting its approach to testing, and this must be done faster, more liberally and extensively, said Prime Minister Lee Hsien Loong in his televised speech in May.
On Jun 16, rapid self-test kits went on sale in pharmacies. These help detect and isolate persons quickly when they are most infectious, and will be a “big help” in slowing the spread of COVID-19, Mr Lee said.
With tests becoming faster and cheaper, routine testing could be done at more workplaces, restaurants and shopping malls, and for individuals like educators and taxi drivers whose jobs involve coming into close contact with many people, he said.
FAQ: What you need to know about the new DIY COVID-19 antigen rapid test kits
Singapore will also contact trace more widely, Mr Lee said, with contact tracers working faster and better because they have more experience, skills and better tools like TraceTogether and SafeEntry.
“I will be looking out for how the testing and contact tracing parts of the strategy change as vaccination increases,” NUS’ Asst Prof Clapham said.
“Once we get to a very high proportion of the population vaccinated, we may worry less about asymptomatic infections, as we don’t have the same risk of these infections leading to outbreaks of severe disease.”
IMPROVING SAFETY MEASURES
Until then, organisations at ground zero of variant clusters continue to ramp up safety measures. Both TTSH and Changi Airport put in place restrictions on people entering their premises and completed at least one round of testing for thousands of employees while also introducing other safety measures.
“We now know many of the cases infected with new variant strains of concern, including B16172, have higher quantities of virus in their secretion,” said Prof Leo, noting that the preventive measures then become “even more important”.
These include keeping the environment clean and well ventilated, as well as reducing human-to-human contact, she added.
Dr Hoi Shu Yin, chief nurse at TTSH, told CNA that the hospital is cleaning and auditing its wards for hygiene more frequently. “We also took steps to improve air ventilation in our wards by retrofitting all general wards and ward toilets with exhaust fans,” she said, adding that high-efficiency particulate air (HEPA) filters have also been installed.
Likewise, Changi Airport’s terminals have been fitted with HEPA filters that prevent stagnant air and ensure constant air flow in a single direction. Airport workers are now segregated according to their COVID-19 exposure risk, with no mingling between zones.
READ: Tan Tock Seng Hospital's Ward 9D to resume admissions after enhancing safety measures
READ: Changi Airport to segregate workers based on COVID-19 exposure risk
Other high-risk places are doing more too. The Singapore General Hospital said staff working in wards are required to wear N95 respirators, rather than surgical masks, for “a better mask fit”.
The hospital is also swabbing non-vaccinated staff weekly and vaccinated staff every two weeks, its director of infection prevention and epidemiology Dr Ling Moi Lin told CNA.
“It is critical that we reduce the transmission of the virus rapidly with good public health measures … such as good hand hygiene and masking, adequate ventilation as well as increasing the percentage of vaccinated persons,” said Dr Ling. “As long as there are viruses circulating, there is an opportunity for variants to develop and we need to remove that opportunity.”
WHAT YOU CAN DO
On a personal level, the experts said the proper wearing of masks that meet filtration standards is integral in fighting back against the more infectious variants.
In mid-May, health authorities recommended that people wear masks with better filtration amid a spike in variant cases and the emergence of new clusters.
These masks, both single-use or reusable, should have at least a 95 per cent bacterial filtration efficiency, said MOH at the time.
NCID’s Prof Leo reiterated that masks should closely and completely cover the nose and mouth. “If we sneeze or cough, do it with the mask on because we rely on the filtration function of the mask to limit the number of particles flowing out into the environment,” she said.

Beyond masks, Prof Leo said the usual measures still apply: Hand hygiene, staying home as much as possible as well as early medical attention and testing.
“It is important to remember prevention measures work hand in hand together. No one preventive measure can work alone,” she added. “Community resilience where everyone is doing their very best is key to combating SARS-CoV-2 that is elusive in nature.”
To overcome the variants, NUH’s Prof Fisher said people should adhere to the same measures, like minimising contact with others, more seriously.
“It’s more about doing all the things that we know and doing them well,” he added. “So it’s actually the same measures – they’re just being (implemented) more aggressively.”
VARIANTS WILL CONTINUE TO EMERGE
Nevertheless, the experts agreed that despite Singapore’s best efforts, different and new variants will probably continue to emerge and re-emerge over time.
New strains that are even more transmissible and less virulent, meaning they cause less severe disease, are “extremely likely” to emerge, said Dr Tambyah.
“After a few years, the virus will probably become like one of the common cold viruses widespread but deadly only to the elderly and vulnerable,” he added.
Dr Tambyah highlighted the Russian flu in the late 19th century as one example of this. It eventually became a seasonal coronavirus now seen regularly by doctors.

The experts stressed that new variant strains arise when viruses evolve to adapt and evade human defences, with each variant bringing different challenges.
“Most experts, including myself, believe that SARS-CoV-2, unlike SARS-CoV (which caused the Severe Acute Respiratory Syndrome), will stay with us,” said Prof Leo. “It will continue to evolve and we humans will continue to develop defence mechanisms such as vaccines and treatment.”
The human versus COVID-19 struggle is “expected to be dynamic” and “occasionally volatile with blips of resurgence” in cases, she said.
“We foresee ongoing restriction-relaxation to achieve some degree of balance allowing the healthcare system to cope with the cases and the entire society to return to the desired state of productivity,” she added.

But Dr Leong at the Rophi Clinic warned against a lapse in measures like wearing masks and safe distancing, highlighting that the coronavirus could “mutate against the vaccine”.
“The weaker we are in this defence, the more likely replication and in turn mutations and variants appear,” he added.
“Disorganised, half-hearted attempts are exactly the prescription for viral mutants.”

