The hidden costs of high dental fees on an ageing population
With research increasingly linking poor oral health and gum disease to broader conditions such as cardiovascular disease, diabetes and osteoporosis, experts say it's worth strengthening financial support for dental care, especially in an ageing society.

Beyond being an indicator of disease, there is growing recognition that oral health affects nutrition, social participation, quality of life, and functional independence, and may contribute to frailty. (Illustration: CNA/Clara Ho)

This audio is generated by an AI tool.


When Madam Amy Lau was first fitted with dentures nine years ago, she decided against replacing her lower teeth at the same time, as she learnt it would cost another S$700 (US$550) on top of the S$500 she had already paid for the upper set.
"At the time, I was doing part-time work and didn't earn much," said Mdm Lau, now 65.
She has since found a full-time position as a kitchen assistant, and last month got a full set of dentures after finding a more affordable option at a heartlands clinic, which also allowed her to pay in instalments.
With only two natural teeth left in her upper jaw now, dentures have made it much easier for Mdm Lau to eat and go about daily life comfortably.
Her dentures cost S$1,271 in total, but as a Community Health Assist Scheme (CHAS) Blue cardholder, she paid about S$500 out of pocket. Even this amount, however, was a tough bullet to bite, she said.
"Paying a lump sum of S$500 is still difficult. I hope that eventually there could be more subsidies for dental care, especially for older folks who are not working," she said.
In October last year, the Ministry of Health (MOH) increased dental care subsidies for Pioneer Generation, Merdeka Generation and CHAS Blue and CHAS Orange cardholders.
CHAS Blue cardholders are households with a monthly income per person of S$1,500 or below, or households with no income and living in homes with an annual value of S$21,000 or below to qualify.
CHAS Orange cardholders are households with a monthly income per person of S$1,500 to S$2,300, or households with no income living in homes with an annual value of S$21,000 to S$31,000.
But experts say that as Singapore's population ages, there is a strong case for further expanding government subsidies and financing support for dental care, with more older adults retaining their natural teeth into their senior years.
There is growing recognition that oral health affects nutrition, social participation, quality of life and functional independence, and may contribute to frailty, said Assistant Professor Cynthia Chen from the National University of Singapore (NUS) Saw Swee Hock School of Public Health.
"Poor oral health can impair chewing and nutrition, which may contribute to physical decline and vulnerability in older adults," said Asst Prof Chen.
During a parliamentary debate on MOH's budget in March 2025, Health Minister Ong Ye Kung noted that a person needs at least 20 natural teeth to chew effectively.
However, only 56 per cent of people aged 55 and above in Singapore have 20 or more natural teeth. A full set is 32 teeth.

THE HIGH COST OF AVOIDING THE DENTIST
Despite the importance of oral health, dental experts told CNA TODAY that cost concerns often lead many people to delay or avoid dental treatment.
Dr Amanda Koh, co-founder and chief clinical director of Kohe Dental and Toofus Dental, said that some patients wait until their teeth become extremely loose or fall out naturally before seeking treatment.
She has also seen patients who have delayed treating gum disease, and eventually had to undergo more major restorative treatments such as overdentures or All-on-X dental implants.
These two treatments are for people who have lost many or all of their teeth, using implants to support either removable dentures or a fixed full set of replacement teeth.
“The challenge is that the cost of waiting can sometimes lead to higher costs later," said Dr Koh. "A condition that may have been simpler to manage earlier can become more complicated if it is left untreated for too long."
Health Minister Ong told parliament during the Budget debate that he had met many residents who chose to have a decayed tooth extracted rather than undergo a root canal, as extraction is cheaper and easier.
"But this is penny wise and pound foolish. We will have fewer and fewer teeth as we grow old if we take this approach. This diminishes our ability to chew effectively, and in our old age affects our nutritional intake," said Mr Ong.


Dr Jonathan Liu, founder and principal dentist of Dentalis Singapore, said that most expensive dental problems do not appear overnight.
They begin as smaller issues, such as plaque, bleeding gums, early decay, cracks, old fillings, grinding, dry mouth, poor access for cleaning, or a missing tooth, that slowly affect the bite.
"If these are caught early, treatment is usually simpler, more conservative and less costly," he said.
As such, Dr Liu, along with other dentists and health experts, said financing support for dental care should not only focus on emergency pain relief. It should also support function, preservation and long-term oral health, he said.
Indeed, among elderly people who spoke to CNA TODAY, several said that the prohibitive costs of dental services deterred them from seeking proper care, or even bothering to find out more about treatment and payment options.
For years, Madam Seng Whay, 78, opted to have painful teeth extracted rather than pursue restorative treatment, as extractions were cheaper and alternatives such as implants and other tooth-preserving procedures were not commonly encouraged at the time.
“Whenever there was tooth pain, I would go and pull it,” said Mdm Seng, who has been wearing dentures since 1986.
Whenever there was tooth pain, I would go and pull it.
She remains reluctant to get a new set because she worries it would be expensive and difficult to get used to.
As for Ms Nancy Lim, 73, uncertainty over costs has deterred her from crowning her front teeth, which were filled many years ago.
“I thought of getting a crown, but I never asked the dentist how much it is,” she said.
Ms Lim said the prospect of repeated dental appointments and a longstanding fear of dental procedures have made her hesitant to ask about the procedure.
This avoidance of dental care among the elderly is a concern. Assistant Professor Charlene Goh, from the NUS Faculty of Dentistry, said studies have demonstrated an association between oral health and systemic issues, such as malnutrition, diabetes and frailty.
“In recent years, increasing attention has been placed on the concept of oral frailty,” she said. The medical condition refers to a decline in mouth and jaw function that can become “a warning sign for systemic decline, including malnutrition, sarcopenia (loss of muscle mass), and a risk for cognitive impairment”.
“Preventive dental care is an important tenet of oral health promotion,” Asst Prof Goh added, noting that reducing the risk of tooth decay and gum disease can help avoid more complex and costly dental treatment later on.
"The mouth is part of the body, and oral health should not be viewed as separate from general health," said Dr Koh from Kohe Dental and Toofus Dental.

HOW DENTAL FEES HURT THE YOUNG TOO
The cost of dental care can be a strain for younger Singaporeans, too, especially when major dental procedures arise unexpectedly.
Ms Bernice Sim, a student at Nanyang Technological University, had severe wisdom tooth pain in the past month, which meant she could not delay surgery. She went to a private dental clinic, where the bill eventually exceeded S$1,800.
“This is the first medical cost that I have incurred that reached four digits… (but) it couldn’t really be avoided,” said the 22-year-old.
Ms Sim said she had to dip into her savings to pay the additional S$300 in out-of-pocket costs, while the surgery effectively wiped out her MediSave balance.
She might have gone to a polyclinic or national dental centre, which offer dental care services at more heavily subsidised rates, but she was in too much pain to wait for an appointment.
In a parliamentary reply in January 2025, MOH said the median waiting time for new appointments for non-emergency basic dental services at polyclinics was about three months, while specialist services at national dental centres had a waiting time of about one month. Emergency cases, however, were seen on the same day.
Other younger patients who opted to seek treatment at private dental clinics spoke of similarly hefty bills. One of them, 42-year-old Jarieul Wong, spent years and thousands of dollars trying to save one tooth.
What began as a slight discolouration in one of the public relations professional's front teeth eventually turned into a five-year dental ordeal that started in 2019, which cost him close to S$10,000, all out of his own pocket.
“I thought it was just discolouration,” he said. “I was shocked at the price.”
He first had to undergo a root canal and replacement work costing about S$4,000, but the treated tooth began darkening again. Multiple dentists told him bacteria might have remained deep within the tooth and that cracks might have formed in the root.
One attempted to save the tooth with bone grafting and other procedures, which cost him about S$2,000, but the treatment was ultimately unsuccessful. On top of that, he was also fitted with a temporary denture, which cost him another S$500.
The dentists he consulted further told him it would cost another S$5,000 to fix the issue, but he did some research on getting treatment overseas and eventually travelled to Bangkok for bridge treatment, which cost about S$2,240, along with airfares.
"I feel relieved (that it is over), but this is just one tooth. I'm not doing major dental work. That is the frustrating part, I'm spending so much on one tooth."
A dental bridge is a treatment that replaces one or more missing teeth by attaching artificial teeth to the natural teeth on either side of the gap.

Meanwhile, Mr Joel Benjamin Chen was 23 years old and serving National Service (NS) when what began as a cavity quickly escalated into a root canal after the decay reached the nerve of his tooth.
Mr Chen remembers the pain as being intense.
“Each time I bit down, there was a sharp jolt of pain,” said the barista, now 27. “Even touching (the tooth) was painful.”
Since the affected tooth was near the front of his mouth, extraction was not a realistic option for him: “For a young guy, having a tooth missing is a confidence destroyer."
Mr Chen said he was relieved that the treatment he received was covered under NS benefits. Outside the military system, he was told the root canal, temporary crown and permanent crown he needed could cost S$2,000 to S$3,000.
But while the root canal procedure itself was covered under NS benefits, Mr Chen still had to pay about S$450 out of pocket for the materials used to make the permanent crown, which was produced by an external laboratory.
At the time, his NS allowance was about S$700 a month, so the S$450 weighed heavily on him.
“If I hadn't been in NS … I would have had to ask my parents to help out financially.”
Mr Chen said the experience has completely changed how he approaches dental health. He now goes beyond basic brushing by flossing his teeth and using mouthwash regularly to avoid ending up in the same situation again.
It's a wise move on his part – research over the years has shown that poor oral health doesn't just affect the mouth; research has linked gum disease and oral bacteria to broader systemic conditions, including cardiovascular disease, diabetes and osteoporosis.
For example, periodontal disease, especially in its more advanced stages such as periodontitis, can be a sign of undiagnosed diabetes, just as diabetes can undermine gum health.
Periodontitis, or gum disease, is a severe infection that damages gum tissue and supporting bone, leading to loose teeth or tooth loss if untreated.
WHY DENTAL CARE IS EXPENSIVE
Singaporeans have long relied on MediSave to offset their medical bills. The scheme was introduced in 1984 as part of the National Health Plan to help citizens build up their savings for future hospitalisation and medical expenses.
Under MediSave, Central Provident Fund contributions are set aside to pay for approved healthcare expenses such as hospitalisation and selected outpatient treatments.
Dr Phua Kai Hong, a health economist and honorary fellow at NUS, said that when the scheme was first crafted, medical care was seen as unpredictable and potentially catastrophic in cost because patients could enter the hospital for what appeared to be a minor issue, only to require major surgery or expensive treatment.
Dental care, by contrast, was viewed as more predictable, preventable and manageable through personal savings.
“Dental health was actually only for preventive care for the very young and emergency care for the very old. Anything beyond that was seen as something people could anticipate and pay for themselves – almost like a luxury good,” he said.
Asst Prof Chen agreed, noting that when MediSave was introduced, its primary purpose was to protect Singaporeans against large healthcare expenses, particularly hospitalisation and major medical treatments, while dental care was generally viewed as a lower-cost expense.
While MediSave can be used for selected major dental procedures such as the surgical placement of dental implants, MediSave contributions are not designed to cover most routine, restorative or orthodontic dental treatment.
Associate Professor Jeremy Lim, from Yong Loo Lin School of Medicine at NUS, noted that “the current financing model was premised on an incomplete understanding of the importance of oral health”.
"Traditionally, dental hygiene was seen as ‘elective’ in the sense that it was nice to have, and extractions and dentures could address neglect."
Today, basic dental care in Singapore is better supported through a range of government subsidies and schemes. Lower- and middle-income Singaporeans can receive subsidised treatment through CHAS, while seniors also receive support through the Pioneer and Merdeka Generation packages.
Still, major gaps remain once patients require more complex restorative treatment, dentists and experts said.
“Basic dental care is better supported today, but many patients only seek help when their condition has already become more complex,” said Dr Koh.
“By that stage, they may need treatment that falls outside basic subsidies or insurance coverage," she said.
Similar structural factors also help explain why dental insurance coverage in Singapore tends to be far more limited than mainstream medical insurance, experts said.
Dr Sunny Leong, head of the work-study programmes at SUSS Academy at the Singapore University of Social Sciences (SUSS), said corporate dental insurance plans are typically structured very differently from medical ones because dental care is seen as highly predictable and routinely used, rather than catastrophic or unexpected.
"Medical insurance is designed for ‘what if’ emergencies, whereas dental benefits manage ‘when’ maintenance," she said.
Since most employees use dental benefits regularly for routine care such as scaling and polishing, insurers and employers tend to treat dental coverage more as a tightly controlled wellness benefit than as traditional insurance protection against large medical expenses.
As a result, corporate dental plans are usually capped and focused on basic procedures, while more complex restorative treatments, such as root canals, crowns, and implants, often remain largely out of pocket.
“Dental care operates on a ‘high-utilisation, low-risk’ model that breaks the traditional maths of insurance,” Dr Leong said.
She explained that insurance often relies on risk pooling, with a large group of healthy people paying premiums to cover the high costs incurred by a small number of people facing unexpected medical events.
Dental care, however, works differently because it is predictable and routinely used.
Since most employees are likely to claim dental benefits each year, insurers generally limit coverage to basic preventive care and impose annual caps on payouts to keep premiums affordable and costs predictable.
The high cost of dental care is also related to the significant overheads needed to operate a dental clinic.
“The main cost drivers are manpower, rent, equipment, lab costs, materials, compliance, and the cost of maintaining proper clinical standards,” Dr Ong Han Yi of Smileplus Dental said.
"We try to avoid being in prime areas to allow ourselves space to keep prices more affordable," said Dr Ong. Smileplus Dental operates two clinics, located in Hougang and Redhill.
He added that rents alone can reach between S$12,000 and S$20,000 a month in some areas of Singapore, forcing clinics to either absorb high overheads or pass on these costs to patients.

RECENTLY INCREASED SUBSIDIES FOR DENTAL CARE
Singapore has gradually expanded dental subsidies over the years as oral health becomes a more pressing issue in an ageing society, with people retaining their natural teeth longer and requiring more complex restorative care.
Subsidised dental care is available through polyclinics and private CHAS clinics, while additional support is provided under the Pioneer and Merdeka Generation schemes.
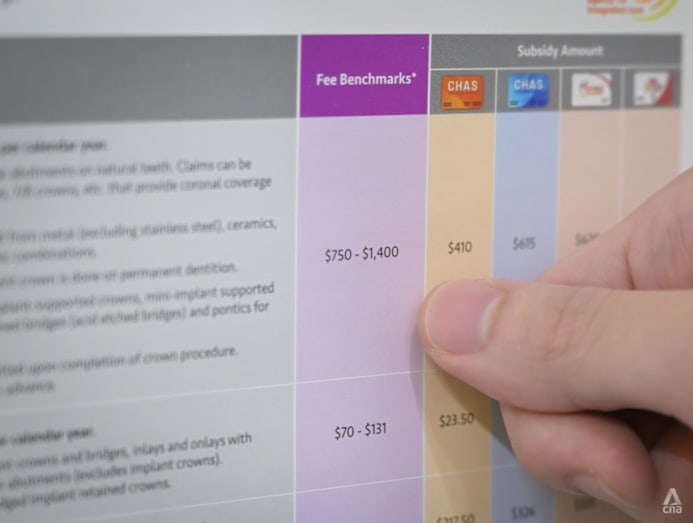
Since October 2025, CHAS Orange cardholders have been eligible to receive a subsidy extension of up to S$45.50 for 10 basic and preventive dental procedures, such as scaling and polishing.
There are increased subsidies for seven restorative dental procedures, including root canal treatment and dentures for Pioneer Generation, Merdeka Generation, as well as for CHAS Blue and CHAS Orange cardholders.
A Pioneer Generation senior can now claim subsidies of up to S$625 for a permanent crown and S$594.50 for a molar root canal treatment. Previously, the subsidies for a permanent crown were between S$137.50 and S$625, and for a molar root canal treatment, between S$266.50 and S$594.50.
Additionally, from June 2026, seniors aged 60 and above will be able to use their Flexi-MediSave to offset up to S$400 a year for root canal treatments and permanent crowns at CHAS dental clinics and public healthcare institutions.
All CHAS dental clinics from mid-2026 will also be required to onboard the Flexi-MediSave scheme. Dental practitioners in CHAS dental clinics will also need to be MediSave-accredited.
Flexi-MediSave is a scheme that allows seniors aged 60 and above to use part of their MediSave savings for approved outpatient treatments, including selected dental procedures from mid-2026.
From Sep 1 this year, CHAS dental clinics will also be required to submit clinical justifications for CHAS subsidy claims that exceed the fee benchmarks set by MOH.
In response to queries from CNA TODAY, MOH said the ministry views oral health as an integral part of overall health and well-being.
"The links between oral health and systemic conditions such as diabetes and cardiovascular disease are well-established," said an MOH spokesperson.
"This is particularly important in the context of an ageing population, where poor oral health can affect nutrition, quality of life and the management of chronic conditions."
Apart from ensuring oral healthcare remains affordable and accessible, MOH said it supports a range of preventive oral health initiatives to promote oral health across all ages.
These include the School Dental Service, which is run in partnership with the Ministry of Education and provides dental care and oral health education for children, as well as Project Silver Screen, which screens seniors aged 60 and above for functional decline, including oral health issues, to enable earlier intervention.
MOH noted that both preventive and restorative dental procedures are subsidised at CHAS clinics and public healthcare institutions. MediSave can also be used to help defray the cost of approved dental surgeries, such as wisdom tooth removals, after subsidies have been applied.
For subsidised patients receiving treatment at public healthcare institutions who continue to face financial difficulties, MediFund may provide additional assistance, added MOH.


FILLING IN THE GAPS
While there is now a stronger case for further expanding support for dental care amid a fast-ageing population, experts cautioned that significantly broadening subsidies or insurance coverage for all dental treatment may not be financially sustainable.
Assoc Prof Lim, from Yong Loo Lin School of Medicine, said funding for dental care is “playing catch-up to a new understanding of oral hygiene”.
But he added that expanding preventive dental care would take time because Singapore has a shortage of dental professionals.
“Even with funding, the numbers that would benefit from preventive dentistry are so large that we have to stage the scaling up,” he said.
Assoc Prof Lim said that even if more funding were available, expanding access to preventive dental care would take time due to manpower constraints in the sector.
"Even with money, there are still shortages of manpower, and hence, despite best intentions, we have to be realistic about how quickly preventive dentistry can be made accessible to everyone."
According to Asst Prof Chen, the main trade-off in expanding dental subsidies is between improving access to care and maintaining the long-term sustainability of healthcare financing.
"More generous subsidies or insurance coverage would likely improve affordability and encourage earlier treatment, but could also increase utilisation and expenditure," she said.
“As the population ages, demand for dental care is expected to increase further,” Asst Prof Chen added, noting that this could also place growing pressure on healthcare spending over time.
Future enhancements are likely to focus on preventive care and support for vulnerable populations, she said.
"This could encourage better oral health while allowing policymakers to manage costs and maintain the sustainability of the healthcare financing system."
Dr Leong of SUSS said Singapore is unlikely to move towards fully subsidised dental care because broader coverage could sharply increase insurance premiums and healthcare spending over time.
“Dental care is highly predictable and utilised by almost everyone for routine cleanings,” she said. “Offering open-ended coverage would cause corporate premiums to skyrocket.”
Instead, she said Singapore’s current approach is designed to keep costs predictable through capped subsidies and tightly controlled dental benefits.

But Dr Leong noted that this also means much of the cost burden ultimately falls on patients themselves.
"Treating oral care as an individualised wellness perk rather than an integrated medical necessity or a state-subsidised right, the Singapore model shifts the financial burden of complex, long-term restorative dental needs almost entirely onto the individual employee," he said.
Dr Leong noted that some countries, such as Japan and South Korea, integrate dental care more deeply into their national healthcare systems, with public subsidies covering a larger share of restorative treatment, dentures and implants.
But she added that these systems also rely on much heavier state involvement and public spending, fundamentally changing the role of employers and insurers in financing dental care.
Associate Professor Sanjeewa Kularatna of Duke-NUS Medical School (Duke-NUS), specialising in health services research and population health, proposed a system with greater subsidies for preventive care and early treatment of dental caries coupled with modest co-payments.
He argued that this would encourage patients to seek treatment earlier, prevent minor dental problems from progressing into more complex and costly conditions, while preserving personal responsibility for their oral health.
“People would be motivated, because they don’t have to spend a lot of money to go to a dentist and get the necessary work done.”
Asst Prof Goh of NUS said prevention remains key to reducing both oral disease and long-term healthcare costs.
“If such treatment can be avoided, the burden on healthcare costs will be lessened.”
Agreeing, Dr Koh said: "Dental care should be seen less as an optional expense and more as part of long-term healthcare planning.”
Ultimately, dental care should not be seen by individuals “only as a cost”, said Dr Liu.
“Good oral healthcare is a form of health maintenance.”
ADDITIONAL REPORTING BY ANG JIE CHUN





